Hyperpigmentation (dark spots, melasma, post-inflammatory marks) affects over 60% of people with Fitzpatrick skin types IV-VI, which includes most Indian, South Asian, African, and Middle Eastern skin tones. Derma rolling shows real promise for skin rejuvenation, but treating pigmentation is a different story. The paradoxical risk of actually making dark spots worse means you need to be extremely careful here.
We put this guide together to help you figure out whether derma rolling can safely reduce your pigmentation, which types actually respond to treatment, and how to prevent PIH (post-inflammatory hyperpigmentation). You will also find safe protocols for darker skin tones and honest advice on when professional intervention makes more sense.
RED FLAG: High Risk of Worsening Pigmentation
Derma rolling for pigmentation carries significant risk of post-inflammatory hyperpigmentation (PIH), especially in darker skin tones. Improper technique, excessive depth, or inadequate sun protection can make dark spots DARKER and more widespread than before treatment. Please read this entire guide before attempting treatment.
Table of Contents
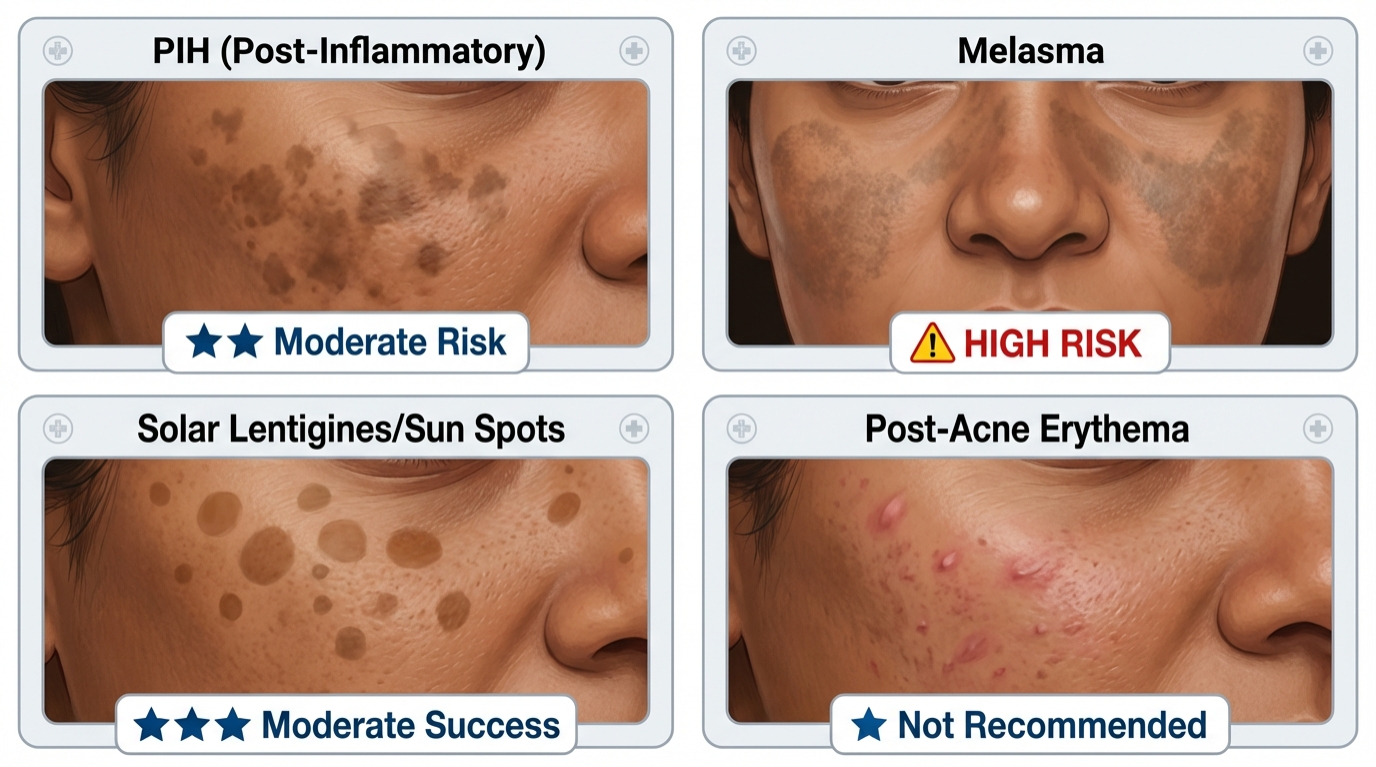
Understanding Hyperpigmentation Types
Not all dark spots are the same, and honestly, this is where a lot of people go wrong. They assume a dark spot is a dark spot, grab a derma roller, and hope for the best. But treatment effectiveness and PIH risk vary dramatically based on pigmentation type and underlying cause. Getting this distinction right matters more than any product you buy.
Post-Inflammatory Hyperpigmentation (PIH)
Cause: Dark marks left after acne, injury, burns, or inflammatory skin conditions. Melanocytes overproduce melanin in response to skin trauma.
Appearance: Flat brown, tan, or dark purple marks that match the shape of previous inflammation. Darkens with sun exposure.
Derma rolling suitability: ⭐⭐ Moderate risk. Can help fade PIH through accelerated cell turnover BUT also carries 30-40% risk of causing NEW PIH from the microneedling trauma itself. Only attempt with strict safety protocols.
Melasma
Cause: Hormonal triggers (pregnancy, birth control, hormone therapy) combined with sun exposure. Deeper melanin deposition in dermis.
Appearance: Symmetrical brown patches on forehead, cheeks, upper lip, chin. Often called "mask of pregnancy."
Derma rolling suitability: ⚠️ HIGH RISK. Melasma is notoriously difficult to treat and highly prone to worsening with ANY skin trauma. Professional treatment (tranexamic acid peels, laser toning) is strongly recommended over at-home derma rolling.
Solar Lentigines (Sun Spots/Age Spots)
Cause: Chronic UV exposure causing localized melanin accumulation. Common after age 40.
Appearance: Well-defined brown spots on sun-exposed areas (face, hands, shoulders, décolletage).
Derma rolling suitability: ⭐⭐⭐ Moderate success. Lighter skin tones (I-III) see 20-30% improvement with 0.5mm needles + vitamin C. Darker skin tones face higher PIH risk with minimal benefit. Laser treatments more effective.
Post-Acne Marks (Erythema)
Cause: Red or pink marks from recent acne breakouts. Temporary increase in blood vessels and inflammation.
Appearance: Pink or red flat marks that fade naturally over 3-6 months without treatment.
Derma rolling suitability: ⭐ Not recommended. These marks resolve on their own. Derma rolling risks converting temporary redness into permanent PIH.
Different types of hyperpigmentation require different treatment approaches and carry varying PIH risks
Does Derma Rolling Work for Pigmentation?
Short answer: Limited effectiveness with HIGH risk in darker skin tones. We wish the answer were more encouraging, but the research paints a complicated picture.
Derma rolling's mechanism for pigmentation reduction relies on a few key processes:
- Accelerated cell turnover: Shedding melanin-laden cells faster through controlled injury response
- Better serum penetration: Brightening ingredients (vitamin C, kojic acid, tranexamic acid) penetrate 80% deeper through micro-channels
- Collagen remodeling: New collagen "pushes" pigmented cells toward surface for shedding
- Reduced melanin clustering: Remodeled skin distributes melanin more evenly, softening the appearance of concentrated dark patches
Clinical Evidence
Published trials report mixed results, and the honest takeaway is that no single study makes a slam-dunk case for derma rolling as a pigmentation treatment:
- 2019 study (Journal of Cosmetic Dermatology): 0.5mm microneedling + vitamin C reduced mild PIH by 28% after 8 sessions in Fitzpatrick III-IV skin
- Korean research (2021): Combination therapy (0.5mm needles + tranexamic acid) achieved 35% melasma improvement BUT 18% of participants experienced PIH worsening
- Indian dermatology consensus (2022): Recommends professional microneedling ONLY for pigmentation in skin types IV-VI, with at-home treatment discouraged due to high complication rates
Critical limitation: The same trauma that stimulates cell turnover ALSO triggers melanin production as a protective response.
In darker skin tones with more active melanocytes, that protective response frequently wins out. The result is often NET DARKENING rather than the lightening you were hoping for.
PIH Risk & Prevention (Critical for Dark Skin)
Post-inflammatory hyperpigmentation is the #1 complication of derma rolling in skin types IV-VI.
Why Darker Skin Has Higher PIH Risk
- More active melanocytes: Darker skin produces melanin more readily in response to ANY inflammation
- Epidermal trauma sensitivity: Even minor injury triggers protective melanin surge
- Longer-lasting marks: PIH in darker skin can persist 1-2 years versus 3-6 months in lighter skin
- Deeper pigment deposition: Melanin deposits into dermis, making it harder to treat
DERM NOTE: The PIH Paradox
You're using derma rolling to REDUCE dark spots, but the treatment itself can CREATE new dark spots. That catch-22 is exactly the reason professional supervision is strongly recommended for darker skin tones. A dermatologist can adjust depth, pressure, and post-care to minimize PIH risk while maximizing benefit.
PIH Prevention Strategies (MANDATORY)
- Start conservatively: 0.25mm needles ONLY for first 6-8 sessions. Never start with 0.5mm+ on pigmented skin.
- Test patch first: Treat small inconspicuous area (jawline) and wait 4-6 weeks to assess PIH response before treating full face.
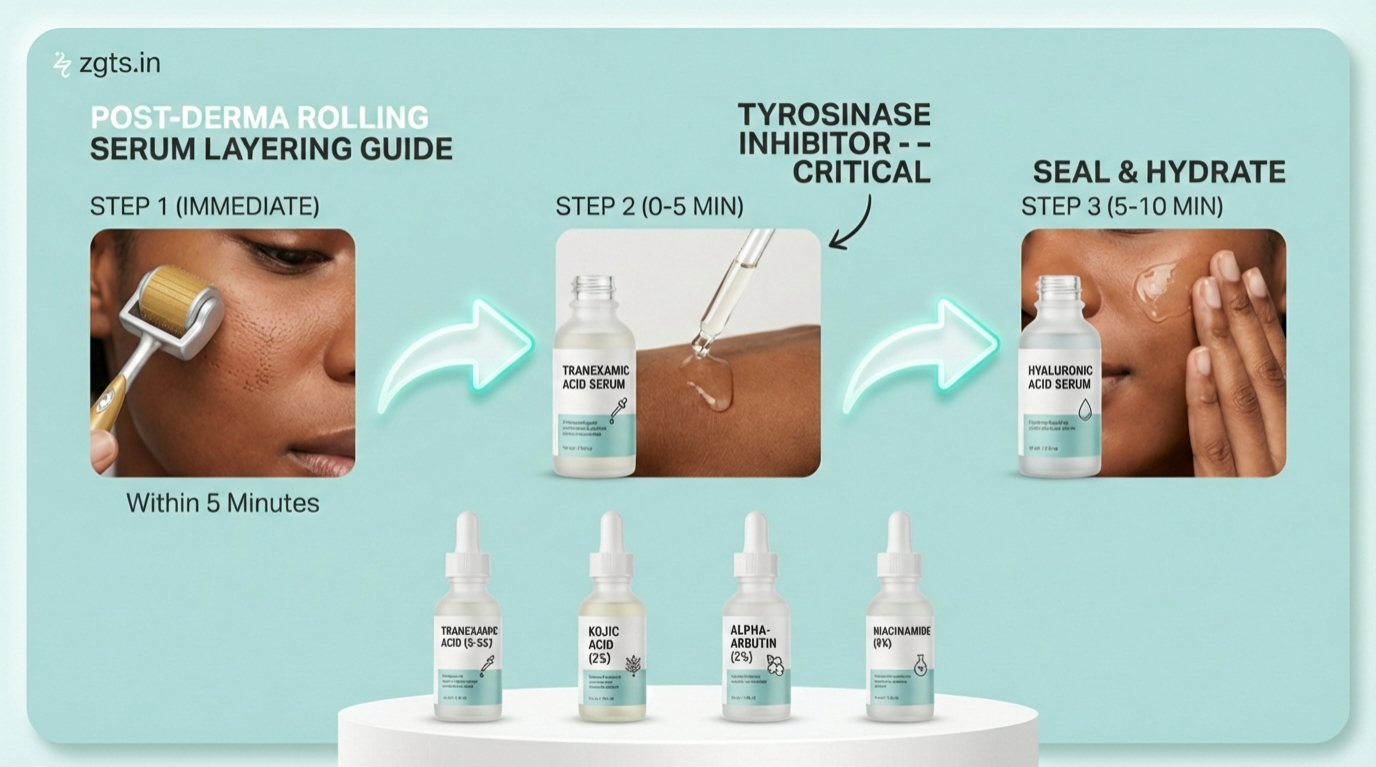
- Tyrosinase inhibitors immediately after: Apply kojic acid (2%), tranexamic acid (3-5%), or alpha-arbutin (2%) within 5 minutes post-treatment to suppress melanin production.
- Strict sun protection: SPF 50+ mineral sunscreen (zinc oxide) EVERY 2 HOURS for 7 days post-treatment. Wear wide-brim hat outdoors. UV exposure is the fastest way to trigger PIH.
- Avoid active ingredients: No retinoids, AHAs/BHAs, benzoyl peroxide, or vitamin C for 5-7 days post-treatment (they increase inflammation risk).
- Monitor closely: Use our treatment tracker to log each session and watch for any darkening. If you notice ANY darkening after a session, STOP immediately and do not resume treatment. See a dermatologist.
Safe Protocol for Pigmentation Treatment
If you decide to attempt derma rolling for pigmentation despite the risks, follow this conservative protocol exactly.
Pre-Treatment (2 weeks before)
- Start daily SPF 50+ mineral sunscreen habit
- Begin using tyrosinase inhibitor serum (kojic acid, tranexamic acid, or azelaic acid) to prepare skin
- Discontinue all exfoliating products (retinoids, acids) 1 week before
- Ensure skin is calm with no active breakouts, irritation, or recent sun exposure
Treatment Day
- Cleanse: Gentle pH-balanced cleanser, pat dry completely
- Disinfect roller: 70% isopropyl alcohol soak for 10 minutes
- Roll with extreme caution:
- LIGHT pressure (lighter than facial treatment)
- Maximum 4 passes per direction (vertical, horizontal, diagonal)
- Total treatment time: 5-7 minutes maximum
- Stop immediately if you see pinpoint bleeding (pressure too high)
- Immediately apply tyrosinase inhibitor: Within 5 minutes, which is CRITICAL for PIH prevention
- Seal with hyaluronic acid: Additional hydration and barrier support
Post-Treatment (7 days)
- Day 1-2: Tyrosinase inhibitor morning/night, gentle cleanser only, SPF 50+ every 2 hours, NO makeup
- Day 3-7: Continue tyrosinase inhibitor, can resume gentle makeup (mineral-based), maintain strict sun protection
- Ongoing: Daily SPF 50+ is non-negotiable for entire treatment course (4-6 months)
Safe treatment technique: light pressure, 4 passes maximum per direction, with immediate tyrosinase inhibitor application
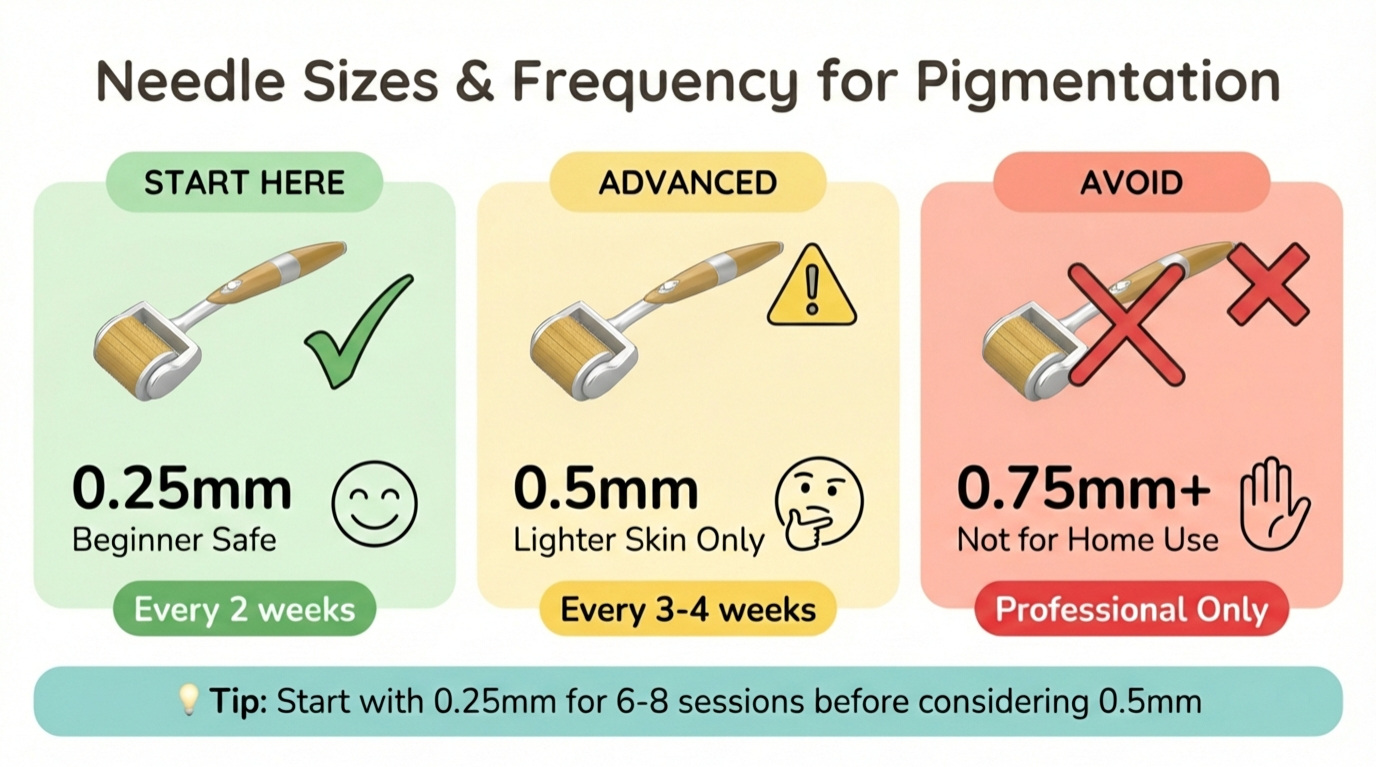
Needle Sizes & Frequency for Pigmentation
| Needle Size | Skin Type Suitability | Frequency | PIH Risk |
|---|---|---|---|
| 0.25mm | All skin types. Recommended starting point for Types IV-VI | Every 2 weeks | Low (10-15%) |
| 0.5mm | Types I-III: Safe. Types IV-VI: Proceed with extreme caution after mastering 0.25mm | Every 3-4 weeks | Moderate (30-40%) |
| 0.75mm+ | DO NOT USE for pigmentation treatment at home | N/A | Very High (60%+) |
Recommended protocol for Indian/brown skin (Types IV-VI): Use our schedule generator to create a safe treatment plan with built-in rest periods.
- Weeks 1-12: 0.25mm every 2 weeks (6 sessions total)
- Assess results at week 12. If NO PIH and seeing 10-15% improvement, may cautiously advance to 0.5mm
- Weeks 13-24: 0.5mm every 4 weeks (3-4 sessions)
- Total treatment course: 6 months maximum. Stop if ANY PIH develops
Combination Therapy with Brightening Serums
Derma rolling ALONE rarely produces significant pigmentation reduction. Combination with proven brightening agents is essential. See our guide to the best serums for derma rolling for a full breakdown of safe actives.
Best Brightening Serums for Post-Treatment
Tranexamic Acid (3-5%)
Mechanism: Blocks plasmin-mediated melanin synthesis. Highly effective for melasma.
Use: Apply immediately after rolling, then 2x daily for 7 days. Continue 1x daily ongoing.
Kojic Acid (2%)
Mechanism: Tyrosinase inhibitor. Prevents melanin formation.
Use: Post-treatment and daily AM/PM. Can combine with tranexamic acid.
Alpha-Arbutin (2%)
Mechanism: Gentler tyrosinase inhibitor. Good for sensitive skin.
Use: Can use immediately post-treatment. 2x daily ongoing.
Niacinamide (5%)
Mechanism: Inhibits melanosome transfer from melanocytes to keratinocytes. Anti-inflammatory.
Use: Safe post-treatment. 2x daily. Can layer with other brighteners.
What to AVOID post-treatment:
- Vitamin C (L-ascorbic acid): Too irritating immediately after. Wait 48-72 hours before reintroducing.
- Retinoids: Increase inflammation risk. Wait 5-7 days.
- Hydroquinone: Prescription-only in many countries. Consult dermatologist before combining with derma rolling.
Results Timeline & Realistic Expectations
Pigmentation fades SLOWLY. If you have been scrolling through social media and seeing dramatic overnight transformations, take those with a heavy grain of salt. Derma rolling accelerates natural cell turnover but cannot produce overnight results. For realistic visual progress examples, see our derma roller before and after guide.
Realistic before and after timeline: 20-40% improvement in superficial pigmentation after 4-6 months of consistent treatment
Weeks 1-6: Minimal Change
Skin may appear temporarily brighter from increased circulation. Dark spots show little visible fading. Some users experience TEMPORARY DARKENING for 1-2 weeks post-treatment (normal inflammatory response).
Weeks 8-12: Subtle Fading Begins
After 4-6 sessions (0.25mm), expect 10-20% reduction in light PIH or sun spots. Melasma shows minimal improvement. Deeper pigmentation largely unchanged.
Months 4-6: Maximum Benefit
Realistic outcome after 8-12 sessions: 20-40% improvement in superficial PIH or sun spots. Complete elimination is unrealistic. Melasma: 10-25% improvement at best (often requires professional treatment).
Factors Affecting Results
- Pigmentation depth: Epidermal (responds better) vs dermal (resistant)
- Skin tone: Lighter skin (I-III) shows faster results with lower PIH risk
- Sun protection compliance: #1 factor in success. Unprotected UV exposure negates all progress
- Serum quality: Medical-grade brighteners significantly more effective
- Underlying cause: Hormonal melasma more resistant than sun-induced spots
When to Avoid Derma Rolling for Pigmentation
Absolute Contraindications
- Active melasma flare (wait until stable for 3+ months)
- History of keloid scarring or abnormal wound healing
- Fitzpatrick skin type VI (very high PIH risk)
- Recent sun exposure or tanning within 2 weeks
- Currently using photosensitizing medications
- Pregnancy or breastfeeding (hormonal influence on pigmentation)
- Active acne or skin infection in treatment area
- Vitiligo or other depigmentation disorders (can trigger Koebner phenomenon)
When to Stop Treatment Immediately
Discontinue derma rolling and see a dermatologist if you develop:
- NEW dark spots appearing after treatment (PIH)
- Existing spots getting DARKER instead of lighter
- Hypopigmentation (white spots) in treated areas
- Persistent redness lasting >48 hours
- Skin infection (increased warmth, pus, spreading redness)
- Scarring or texture changes
Better Professional Alternatives for Pigmentation
Look, we sell derma rollers, so take this for what it is worth: for significant pigmentation, professional treatments genuinely offer a better risk-to-benefit ratio than at-home derma rolling. Sometimes the best advice is knowing when a tool is not the right fit.
Recommended Professional Treatments
Tranexamic Acid Mesotherapy
Intradermal injections of tranexamic acid directly into pigmented areas. Highly effective for melasma (50-70% improvement).
Cost: ₹3,000-₹6,000 per session | Sessions: 4-6 monthly
Q-Switched Nd:YAG Laser Toning
Gold standard for melasma and deep pigmentation in darker skin. Minimal downtime. 60-80% improvement typical.
Cost: ₹4,000-₹10,000 per session | Sessions: 6-10 biweekly
Chemical Peels (Glycolic, Kojic, TCA)
Controlled exfoliation removes pigmented layers. Multiple peel types for different pigmentation depths.
Cost: ₹2,500-₹6,000 per session | Sessions: 4-8 monthly
Professional Microneedling with RF
Microneedling combined with radiofrequency energy. More controlled than at-home rolling with better pigmentation results.
Cost: ₹8,000-₹15,000 per session | Sessions: 3-5 monthly
Frequently Asked Questions
Can derma rolling make pigmentation worse?
Absolutely yes. This is the #1 risk. Post-inflammatory hyperpigmentation (PIH) occurs in 30-60% of darker-skinned individuals who use derma rolling for pigmentation treatment. The same micro-injuries that stimulate cell turnover also trigger melanin production as a protective response. If your skin has a strong melanin response, you'll end up with MORE dark spots than you started with.
Which needle size is safest for pigmentation?
0.25mm is the safest starting point for ALL skin types, especially Fitzpatrick IV-VI. Our derma roller size calculator can help you confirm the right needle size for your skin type and concern. Use 0.25mm exclusively for first 6-8 sessions (3-4 months). Only advance to 0.5mm if you see NO PIH development and are achieving some benefit. Never use 0.75mm+ for pigmentation treatment at home. That depth belongs in a professional setting only.
How long until I see results on dark spots?
Realistic timeline: 8-12 weeks for first noticeable lightening (10-20% improvement), 4-6 months for maximum benefit (20-40% improvement). Complete elimination of established pigmentation is unrealistic with at-home derma rolling alone. Superficial PIH responds better than deep melasma or sun damage.
Is derma rolling effective for melasma?
Very limited effectiveness with HIGH risk. Melasma is notoriously difficult to treat and extremely sensitive to any skin trauma. At-home derma rolling for melasma carries 40-50% risk of worsening. Professional treatments (tranexamic acid mesotherapy, Q-switched laser toning) are strongly recommended instead. If you attempt derma rolling: 0.25mm ONLY, strict sun avoidance, mandatory tyrosinase inhibitors, and professional supervision.
What serums should I use after rolling for pigmentation?
Priority #1: Tyrosinase inhibitors applied within 5 minutes post-treatment:
- Tranexamic acid (3-5%), best for melasma
- Kojic acid (2%), a strong melanin blocker
- Alpha-arbutin (2%), the gentler option
- Niacinamide (5%) for anti-inflammatory + brightening effects
Wait 48-72 hours before reintroducing vitamin C or retinoids. Layer with hyaluronic acid for hydration.
Is derma rolling safe for Indian/brown skin pigmentation?
Proceed with EXTREME caution. Indian skin (typically Fitzpatrick IV-V) has 3-4x higher PIH risk than lighter skin tones. Recommendations: (1) Mandatory test patch on jawline first, (2) Start with 0.25mm ONLY, (3) Use lightest possible pressure, (4) Apply tyrosinase inhibitors immediately post-treatment, (5) Strict SPF 50+ every 2 hours, (6) Consider professional treatment instead for significant pigmentation. If you see ANY new dark spots after first session, STOP and see a dermatologist.
Can I use derma roller on old acne marks?
Depends on mark type. RED/PINK post-acne erythema: No, because these fade naturally and derma rolling risks converting them to permanent PIH. BROWN post-acne PIH: Maybe. Derma rolling can help accelerate fading BUT also carries risk of making them darker. Use 0.25mm, test patch first, strict sun protection. For depressed acne SCARS (not marks), see the acne scars guide.
Should I see a dermatologist before treating pigmentation?
Strongly recommended, especially for: (1) Fitzpatrick skin types IV-VI, (2) Melasma or hormonal pigmentation, (3) Extensive or deep pigmentation, (4) History of PIH or keloid scarring, (5) Uncertainty about pigmentation cause. A dermatologist can diagnose pigmentation type, assess PIH risk, recommend most effective treatment, and provide professional microneedling with proper safety protocols if appropriate. ₹1,000-₹2,000 consultation can save you from ₹50,000+ in corrective treatments for PIH complications.
Reviewed by Dr. Priya Mehta, MD Dermatology
MBBS, MD Dermatology. 12+ years clinical experience treating pigmentation disorders in Indian skin types (Fitzpatrick IV-VI). This guide reflects current research-backed practices and critical PIH prevention protocols.
Related Guides
Derma Roller for Face: Complete Guide
Full facial microneedling guide covering all skin concerns and proper technique.
Derma Roller for Dark Circles
Safe protocols for delicate under-eye area with critical safety warnings.
Derma Roller for Acne Scars
Research-backed protocol for treating atrophic acne scars with microneedling.
10 Derma Rolling Mistakes to Avoid
Critical errors that cause PIH and other complications.
Derma Roller for Dark Knees & Elbows
Targeted protocols for treating hyperpigmentation on body areas like knees, elbows, and other darkened patches.